Article Text

Abstract
Objective The irritable bowel syndrome (IBS) population is heterogeneous, harbouring a variety of abdominal symptoms. Therefore, IBS is often termed a ‘diagnosis of exclusion’. Chronic abdominal wall pain (CAWP) is a poorly recognized entity, frequently caused by the anterior cutaneous nerve entrapment syndrome (ACNES). Some patients may be misdiagnosed because IBS and CAWP share symptoms. Aim of this study was to construct and validate a questionnaire to distinguish patients with CAWP (including ACNES) patients with IBS.
Design A questionnaire was designed of 17 ACNES characteristic items obtained from ACNES patients (n=33) and expert opinion of two specialized surgeons. Eleven IBS-related items (‘Rome III’ criteria) were added leading to a questionnaire containing 28 items. This was validated in a ‘gold standard’ ACNES group (successfully operated ACNES patients, n=68) and a ‘prospective’ IBS group (n=64) as well as in a ‘prospective’ ACNES group (n=47). Distinctive power of individual items was analyzed by χ2. Reliability was tested with Crohnbach's α. ROC curve was used to determine cut-off values.
Results Eighteen of 28 items were significantly distinctive (p<0.01) between ACNES and IBS patients leading to an 18-point ACNES score with good internal consistency (α=0.85). Cut-off value of 10 points resulted in 94% sensitivity, 92% specificity and areas under the curve (AUC) of 0.98. Evaluation of the prospective ACNES group led to 85% sensitivity, 92% specificity and AUC 0.95 indicating high discriminative properties of the questionnaire.
Conclusions This novel questionnaire may be useful and valid as a simple tool distinguishing patients harbouring a CAWP syndrome from those having IBS.
- ABDOMINAL PAIN
- FUNACTIONAL ABDOMINAL PAIN
- FUNCTIONAL BOWEL DISORDER
- IRRITABLE BOWEL SYNDROME
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Objective
Irritable bowel syndrome (IBS) is a syndrome that is characterised by spells of abdominal discomfort and pain. According to the Rome III criteria, the diagnosis is based on clinical symptoms in the absence of structural or tissue abnormalities. IBS patients are defined by reporting abdominal complaints at least 3 days per month in the previous 3 months. Moreover, the diagnosis is probable if two or more of the following criteria are fulfilled. The onset is associated with a change in frequency and/or appearance of stool, whereas symptoms are attenuated after defecation.1
Due to the descriptive and general character of these Rome III criteria, the current IBS patient population is heterogeneous, harbouring a broad variety of abdominal symptoms. As a consequence, IBS is often termed a ‘diagnosis of exclusion’.2 Estimations on the prevalence of IBS in The Netherlands may vary from 5% to 20% in an average community. Approximately one of three IBS patients requests medical help.3–6 Consequently, some half a million Dutch people are calculated to require treatment for IBS.
Chronic abdominal pain (CAP) is usually thought to arise from a diseased viscus. However, CAP may also be caused by an abnormality situated in the wall of the abdomen. A common cause of this latter category is the anterior cutaneous nerve entrapment syndrome (ACNES). ACNES is caused by entrapment of branches of intercostal nerves (Th 8–12) causing severe CAP. Myofascial pain and radiculopathy are considered less frequent causes of abdominal wall pain.7 ,8 As a tertiary referral centre, our research group is especially interested in CAP due to ACNES. Carnett's statement some 85 years ago that ‘the ACNES problem never received merited recognition in medical literature’ still holds true at present.9–15 The diagnosis of ACNES is based on the finding of a constant site of tenderness that is superficially located, with a small area of maximal tenderness that can be localised with a fingertip (trigger point). The tenderness is invariably increased after abdominal muscle tensing using the Carnett's test. Moreover, a small area of somatosensory alterations surrounding the trigger point is often found in ACNES, possibly allowing for a discrimination between a myofascial cause and a radicular cause of the pain.9 ,11 ,16–19 The diagnosis of ACNES can be substantiated by a subfascial injection of 1% lidocaine, typically leading to significant pain reduction after 15–20 min.20 Abnormalities in blood and organ tissues are practically always absent in ACNES patients. Our group recently evaluated a diagnostic work-up protocol and treatment regimen in 139 consecutive patients with suspected ACNES. Local trigger point injections appeared to be long-term effective in one-third of the patients. Surgical neurectomy was effective in approximately two-thirds of the refractory patients. Some 80% of the entire ACNES population reported total or substantial pain relief in the long term.20
As our experience with unravelling the diagnosis in patients with CAWP is growing, we were confronted with some patients harbouring ACNES although previously diagnosed with IBS. The aim of the present study was to develop and validate a questionnaire that may be used to differentiate between IBS and CAWP. We hypothesised that the novel questionnaire may allow a discrimination between various patient populations having CAP.
Design
Setting
The study was coordinated by members of the surgical department and was performed in outpatients departments of gastroenterology and surgery of the Máxima Medical Centre (MMC) in Veldhoven, The Netherlands. The MMC is an 865-bed community hospital serving a population of approximately 350 000–400 000. It is a tertiary referral centre for abdominal wall and groin pain syndromes.20–27
Development of questionnaire
The preliminary questionnaire was composed in November and December 2010 by input from two focus groups and the input from IBS literature. The first focus group consisted of 70 ACNES patients who had undergone successful surgery between 2003 and 2008. They were randomly selected to contribute to the development of the questionnaire. They were requested via an accompanying letter to describe in detail all of the symptoms they had experienced in the period before surgery. The second focus group consisted of two surgeons skilled in diagnosing and treating ACNES. They were invited to report typical symptoms from a professional point of view (RMR and MRS). They both independently provided a list containing what they considered typical complaints reflecting the syndrome of ACNES. Data obtained from both focus groups were used to identify the most ACNES-sensitive questions that were subsequently used in the questionnaire. This was complemented by inserting typical IBS-related questions obtained from three different sources (Birmingham IBS questionnaire, Rome III criteria, Dutch IBS interest group).28–30 All questions were closed-ended, dichotomous (‘yes’, ‘no’) or 4-point Likert scale questions (‘mostly’, ‘regularly’, ‘sometimes’, ‘never’).
Validation of questionnaire
Between February and July 2011 three patient populations were utilised for validation. The first population consisted of a group of ACNES patients who had demonstrated a favourable response to surgery defined as a greater than 50% reduction in pain (measured by visual analogue scale) or a more than 2 point reduction on a 5-point verbal rating scale between 2003 and 2011 (‘gold standard’ ACNES group). This definition was considered ‘gold standard’ in the absence of an alternative one. To obtain this information, a short survey investigating complaints before and after surgery was added to the questionnaire. This first validation population partly overlapped with the population used for questionnaire development. They completed the questionnaire by paper or by the use of the web-based questionnaire from the ThesisTools system. A reminder was sent after 4 weeks if the participant remained unresponsive. Inclusion ended 3 months after the first contact. Responses with more than one missing item were excluded from analysis.
To overcome a possible shortcoming associated with the retrospective character of these treated ACNES patients, a second population of newly diagnosed ACNES patients who presented to the surgical outpatients department was also included for validation purposes (‘prospective’ ACNES group). They were diagnosed between May and July 2011 and completed the questionnaire before visiting the specialist in the outpatients department. The diagnosis of ACNES was confirmed in all individuals by one of the two expert surgeons.
The third population used for validation consisted of a cohort of consecutive patients with a suspected diagnosis of IBS presenting at the gastroenterological outpatients department (‘prospective’ IBS group). Patients were prospectively included between April and May 2011 and completed the web-based survey. Four weeks after the inclusion of these new IBS patients, diagnosis based on the Rome III criteria was re-checked for confirmation.
Calculations
Data analysis was performed using SPSS V.18.0 for MacOS X. During the validation phase, two different steps were executed. First, Likert scale questions were dichotomised before analysis. ‘Mostly’ and ‘regularly’ were interpreted as a positive answer, whereas ‘sometimes’ and ‘never’ were interpreted as a negative answer. Subsequently, the distinctive power of each of both ACNES and IBS items of the questionnaire were measured using χ2 analysis. A less than 0.01 χ2 cut-off point was used. Non-distinctive questions (χ2>0.01) were excluded from the questionnaire. The reliability of the questionnaire was determined using Crohnbach's α. An α>0.9 is considered excellent, α>0.8 is good, α>0.7 is acceptable, α>0.6 is questionable, α>0.5 is poor and α<0.5 is unacceptable.31
A second step was to develop a scoring algorithm for the questionnaire. Two scenarios were evaluated using results from the gold standard ACNES group and from the prospective IBS group. In the first scenario, a simple algorithm was evaluated contributing one point to each question. In the second scenario, points were given based on the distinctive character of a question. The grade of distinctive character was determined by the risk rate of a question. One point was given for a risk rate between 1 and 2.5, two points for a risk rate between 2.5 and 5, and three points for questions with a risk rate greater than 5. Each ACNES-related question received point(s) for a positive answer, whereas an IBS-related question scored point(s) for a negative answer. Patients with a high score were likely to have ACNES, whereas low scores were attained by a typical IBS patient. Cut-off values and discriminating values (sensitivity and specificity) were tested in both ACNES groups using a receiver operating characteristic curve. In the end, a final scoring algorithm was constructed.
Results
Development of questionnaire
The response of 33 ACNES patients (response rate 47%) combined with the opinion of both surgeons led to 17 questions that were deemed sensitive and distinctive for ACNES. A total of 11 IBS-related questions was added resulting in a preliminary 28-item questionnaire. ACNES and IBS questions were sequenced in random order. Twenty-two of the 28 questions investigated pain (course over time n=3, type n=5, localisation n=7, provocative factors n=7), whereas six questions were concerned with other symptoms. Twelve questions were dichotomous, whereas the remaining 16 were 4-point Likert scale questions.
Validation of questionnaire
Subjects
In the gold standard ACNES group, a total of 101 responses was obtained from 130 ACNES patients (response rate 78%). Of these 101 patients, 73 subjects were successfully treated (success rate 72%). As five responders were excluded due to missing items, answers of 68 questionnaires were eligible for analysis (female 81%, age 48±19 years). In the prospective ACNES group, 83 patients suspected of ACNES and visiting the outdoor department of surgery were eligible for validation. As 36 patients were excluded (questionnaire completed after rather than before diagnosis (n=21), uncertain moment of questioning (n=3), other diagnosis (n=8), missing items n=4), questionnaires of 47 remaining subjects with the diagnosis of ACNES were eligible for analysis (female 79%, age 46±17 years). In the prospective IBS group, a population of 66 subjects was drafted from the IBS-group. As two patients were excluded (haemorrhoids n=1, ACNES n=1), a cohort of 64 IBS subjects was eligible for analysis (female 69%, age 50±6 years, Table 1).
Demographic data of validation groups
Definitive form of questionnaire
Some 18 of 28 items showed sufficient discriminative properties between the gold standard ACNES group and prospective IBS patient group (χ2<0.01). This set of 18 items included 11 ACNES and seven IBS questions. In this final set of questions, 14 questions investigated pain (course over time n=1, type n=3, localisation n=5, provocative factors n=7), whereas four questions concerned additional complaints. The 18 questions with distinctive character had a good internal consistency (α=0.85). These properties allowed for the calculation of a total score. Table 2 shows discriminating symptoms associated with either ACNES or IBS.
Discriminating items in the questionnaire
Scoring algorithm
The first ‘one point per item’ scenario led to a minimal score of 0 and an 18 points maximum score, whereas the second scenario had a maximum score of 26 points. Both scenarios were tested for sensitivity and specificity at different cut-off values. As the more complicated scenario 2 conferred no beneficial qualities at the best cut-off value (scenario 1: >10 points; sensitivity 0.94, specificity 0.92 vs scenario 2: >13 points; sensitivity 0.93, specificity 0.95), the simple one point per question scenario was chosen.
Cut-off value
Any test cut-off point must be chosen on the basis of a hypothesis. As knowledge about ACNES is scarce and a minimal prevalence (some percentages) in the IBS-group was expected, the questionnaire should have optimal identification properties. Consequently, such an identification tool needs high specificity. A 10 points cut-off value provides an optimal 0.94 sensitivity, combined with 0.92 specificity.
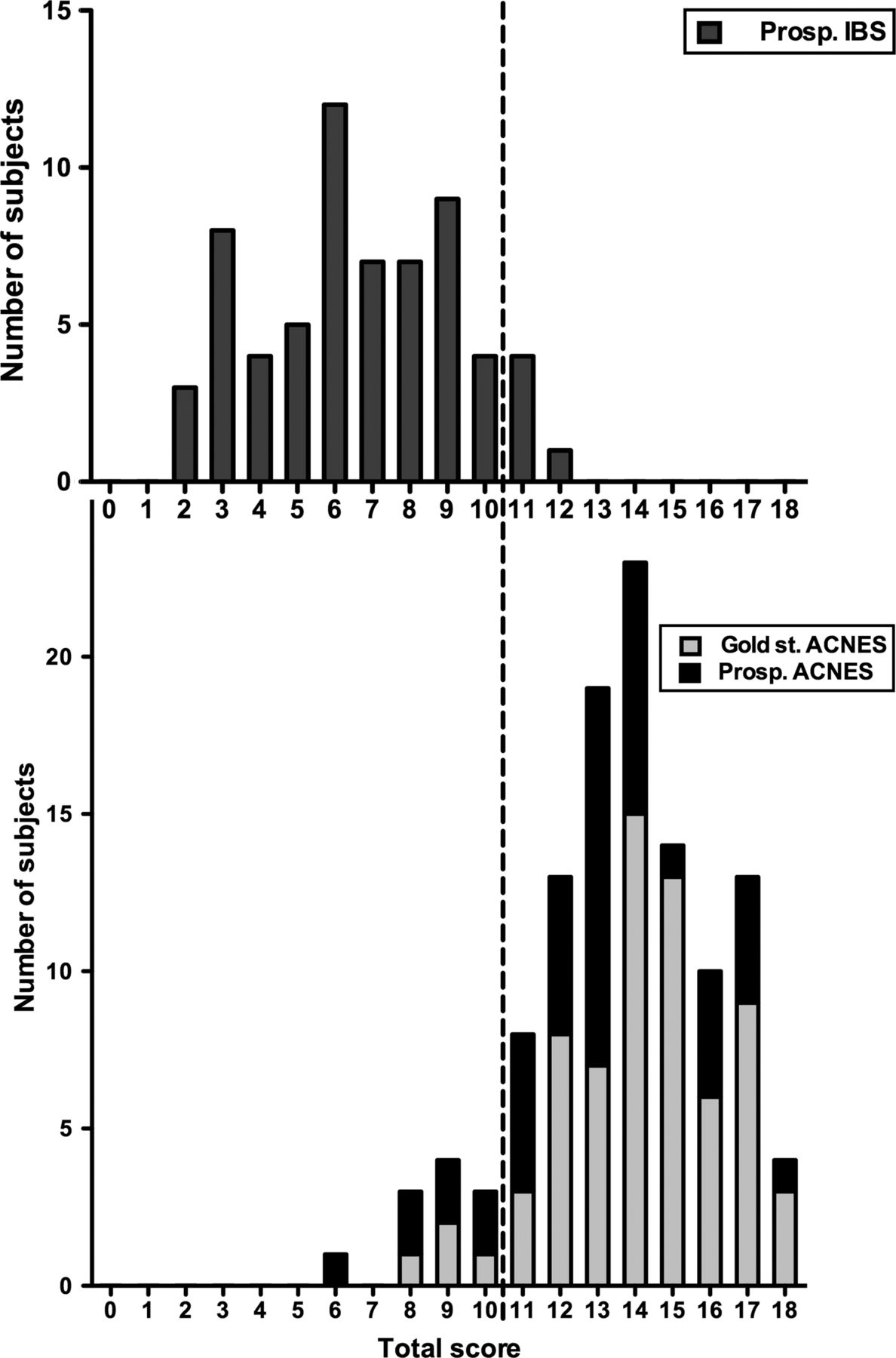
There was a slight reduction in the prospective ACNES group, but the test characteristics were still satisfactory (table 3). Sensitivity was 0.85 for a 10 points cut-off value in this group. Calculated receiver operating characteristic curves of both the gold standard ACNES group and the prospective ACNES group give outstanding areas under the curve (AUC), representing an excellent diagnostic test. The AUC of the gold standard group is 0.98, and the AUC of the prospective ACNES group is 0.95. Scores of all subjects are depicted in the combined histogram (figure 1).
Characteristics of questionnaire with different cut-off values in the prospective ACNES-group compared with the gold standard ACNES group

{kind=link}
Scores of 64 irritable bowel syndrome (IBS) patients (top figure). In the lower figure scores of 68 gold standard (Gold st.) anterior cutaneous nerve entrapment syndrome (ACNES) patients and 47 prospective (Prosp.) ACNES patients. The vertical line is the cut-off value (>10 points).
Discussion
The present study describes a stepwise development and validation of a novel diagnostic tool for the identification of potential ACNES patients within an IBS population. The results indicate that a simple 18-item questionnaire has a 0.94 sensitivity combined with 0.92 specificity. How should these test characteristics be interpreted? Test performance of nationwide screening programmes used for breast and cervix cancer demonstrates sensitivity varying from 0.33 to 0.91 combined with a 0.81–0.99 specificity.32–35 The qualifications of the present CAWP/ACNES questionnaire seem substantially better, whereas its accuracy is excellent (AUC 0.98). Furthermore, a strong internal consistency (α=0.85) contributes to the power of the questionnaire as an identification tool.
A strong point of the present study is the validation in two separate populations of ACNES patients, a retrospective ‘gold standard’ and a ‘prospective’ ACNES group. Answers on four of the definitive 18 questions appeared significantly different (χ2<0.01) between these two groups. As three of these items were IBS-specific questions, it may seem that ACNES patients in the prospective group are more convinced of a visceral cause of their abdominal symptoms. These findings also suggest that information bias combined with recall bias probably played a role in the slight reduction of these test characteristics in the gold standard group compared with the prospective group.
Comparing answers of both groups of ACNES with answers derived from the IBS patients indicated that the discriminating character of the prospective ACNES group was slightly inferior. More specifically, two questions appeared less distinctive (χ2>0.01) compared with their performance in the retrospective gold standard ACNES group. Both items were IBS-related items (‘The stool has an abnormal consistency’ and ‘I feel urgent need for bowel movement without producing stool (incomplete defecation)’). However, as both questions still had significant distinctive properties (<0.05), they were not removed from the ultimate 18-item questionnaire. These observations are in line with the presence of ‘pseudo-visceral symptoms’ that ACNES patients occasionally report.36 ,37 The patient's conviction of a visceral origin of pain complicates the process of diagnosing ACNES in daily clinical practice.
All questions of the Dutch questionnaire were translated into the English language as depicted in table 2. Officially, linguistic validation should be performed before this questionnaire can be used in a language other than the original language.
The current study harbours flaws. Interpretation is limited by selection bias. Although a contemporary IBS population probably includes a broad range of patients presenting to various healthcare providers including general practitioners, the present questionnaire is only validated with IBS patients presenting at the gastroenterology outpatients department. It may be possible that general practitioners are confronted with a different subpopulation of alleged IBS patients presenting with a slightly different pattern of intestinal symptoms. We are currently engaged in a study investigating the test characteristics of the ACNES questionnaire in IBS patients presenting to a number of general practices.
Another flaw of the study is caused by the differential diagnosis of CAWP. When the present study was designed, the authors were convinced that ACNES and CAWP were (almost) identical. In other words, it was thought that CAWP was practically always caused by ACNES. The fact that some patients diagnosed with ACNES (albeit a minority) did not demonstrate altered skin sensibility urged us to assume that the differential diagnosis of CAWP harbours more entities including myofascial pain or radiculopathies. To facilitate understanding of the present study, we chose to use the terms ACNES and CAWP interchangeably.
A substantial number of patients with functional gastrointestinal disorders also report abdominal wall pain. The present questionnaire will have less discriminating power in this subpopulation. On the other hand, if the abdominal wall problems play a prominent role in the patient's pain experience, there is a reasonable chance that this individual is identified after completing the questionnaire. This is particularly true as 11 of the 18 items are obtained from ACNES patients (‘ACNES/CAWP-specific items’). In addition, most items (14 of 18) investigate issues of pain, whereas abdominal wall syndromes are mainly characterised by pain and not by functional complaints.
Despite explicit guidelines and criteria, clinicians often consider IBS a diagnosis of exclusion. Surprisingly, no guideline on IBS reported on findings obtained during a standard physical examination. On the other hand, ACNES is preferentially diagnosed after a simple but proper physical examination. A significant number of patients may be incorrectly burdened with an IBS diagnosis, even more so if pseudo-visceral complaints are experienced. The present questionnaire may prove a valuable tool for the identification of patients with CAWP wrongly assumed as having IBS. The tool may be relevant for several groups of specialists including gastroenterologists and general practitioners. Moreover, other specialists may also find this questionnaire helpful in the evaluation of patients with chronic abdominal discomfort.
Conclusion
A simple 18-item questionnaire may possibly distinguish patients who potentially have CAWP, and in particular ACNES, from a population diagnosed with IBS.
Key messages
What is already known on this topic
-
The current IBS population is heterogeneous harbouring a broad variety of abdominal symptoms.
-
Chronic abdominal wall pain (CAWP) is a frequently missed diagnosis.
-
A common cause of CAWP is the anterior cutaneous nerve entrapment syndrome (ACNES).
What this study adds
-
The developed questionnaire is a useful tool to identify patients with abdominal wall pain.
-
Newly diagnosed ACNES patients tend to report visceral symptoms.
How might it impact on clinical practice in the foreseeable future?
-
Using this novel tool may allow for identification of patients that suffer from pain originating in the abdominal wall.
References
Footnotes
-
Contributors TvA: study concept and design, acquisition of data, analysis and interpretation of data, drafting of the manuscript, critical revision of the manuscript for important intellectual content, statistical analysis; OBB: drafting of the manuscript, critical revision of the manuscript for important intellectual content; JTK: drafting of the manuscript, critical revision of the manuscript for important intellectual content, acquisition of IBS patients at the gastroenterology department; MRS: drafting of the manuscript, critical revision of the manuscript for important intellectual content, statistical analysis, study supervision; RMR: study concept and design, drafting of the manuscript, critical revision of the manuscript for important intellectual content, statistical analysis, study supervision.
-
Funding The study was funded by a grant from the Stichting Hart- en Vaatziekten Zuid Nederland.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/